Subtitle
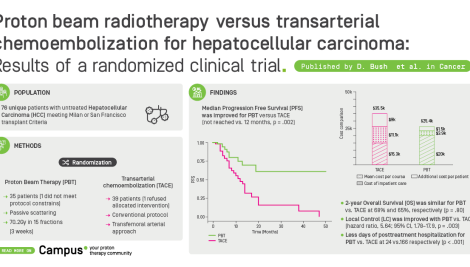
Phase III randomized trial of intensity-modulated proton therapy (IMPT) versus intensity-modulated photon therapy (IMRT) for the treatment of head and neck oropharyngeal carcinoma (OPC)
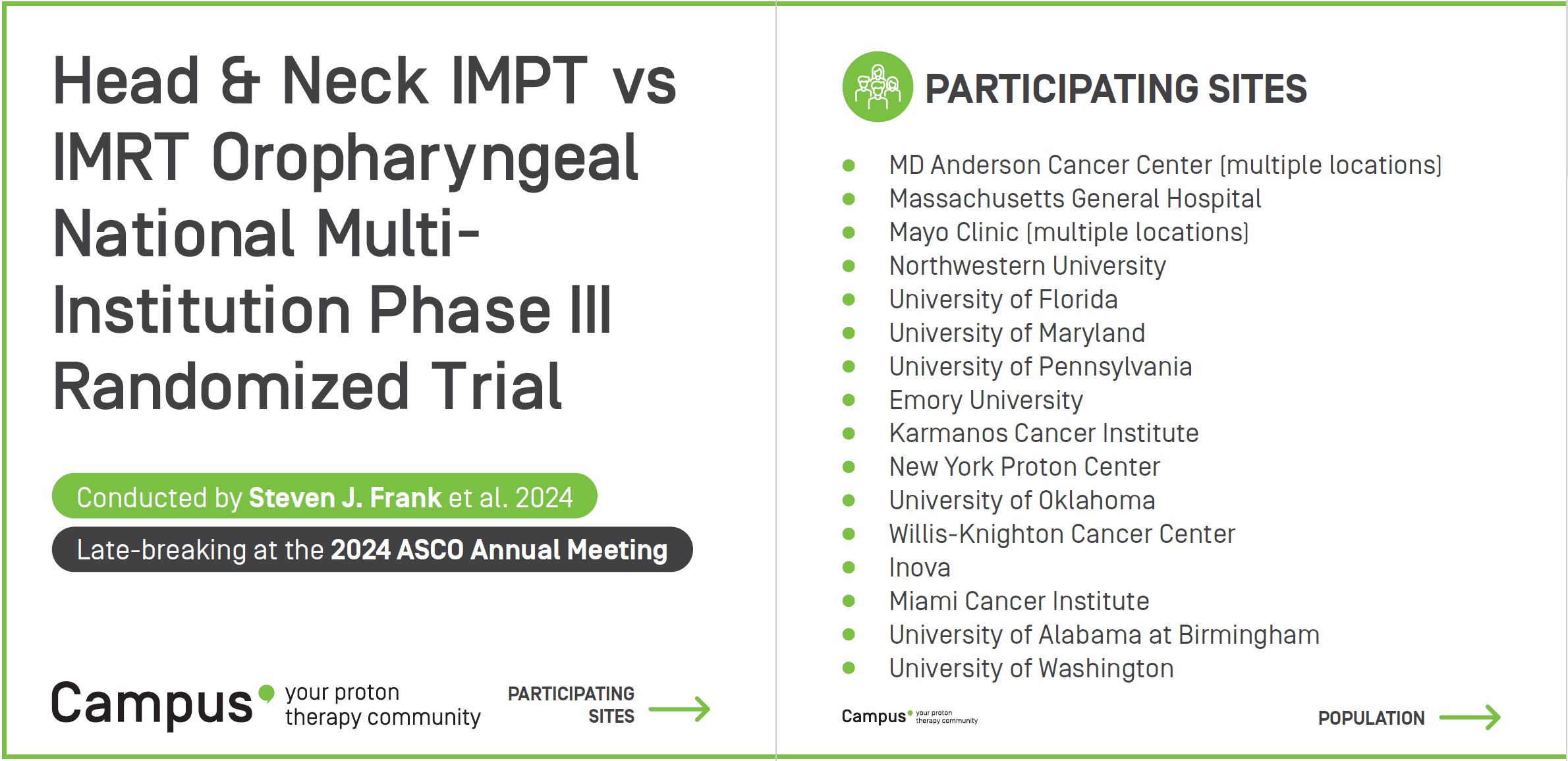
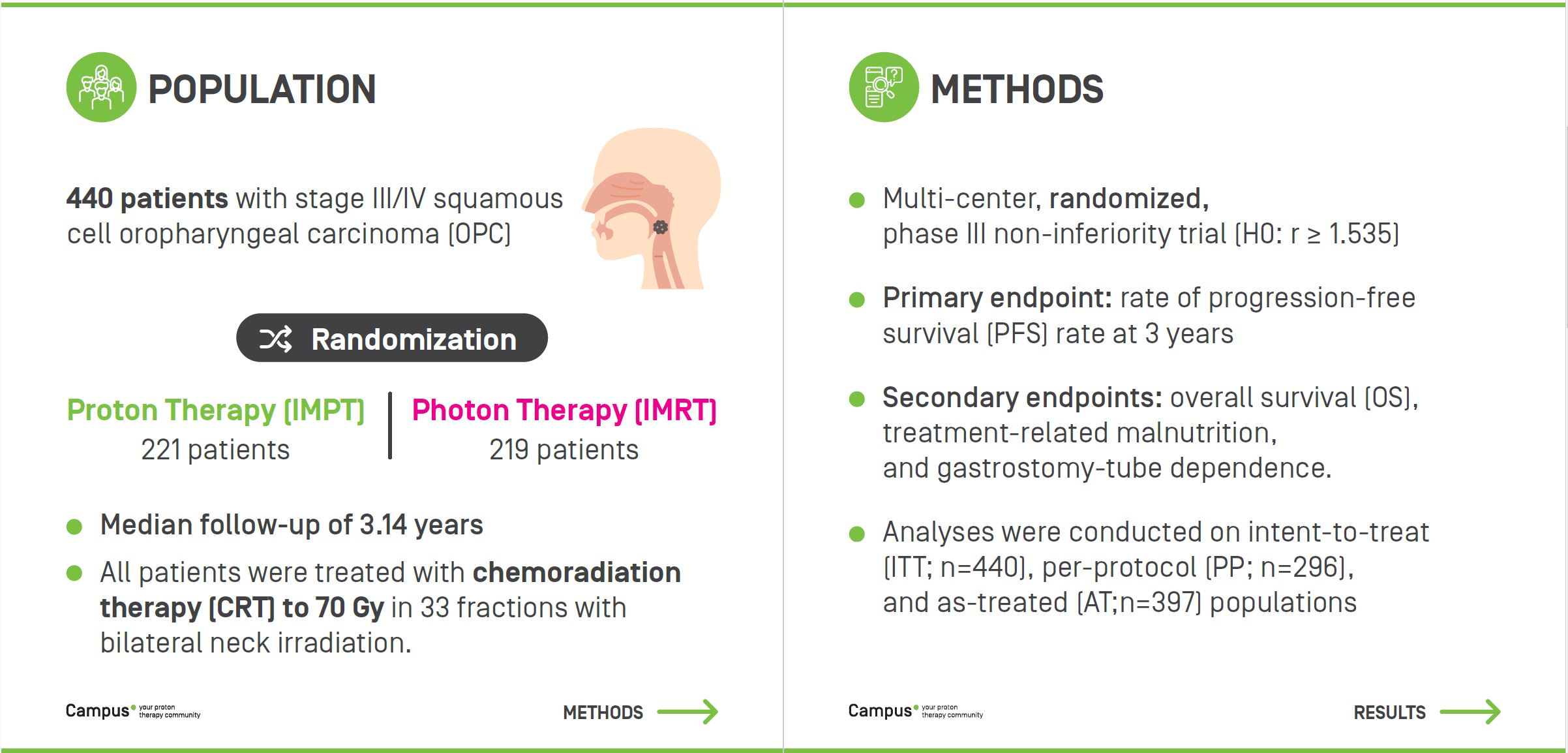
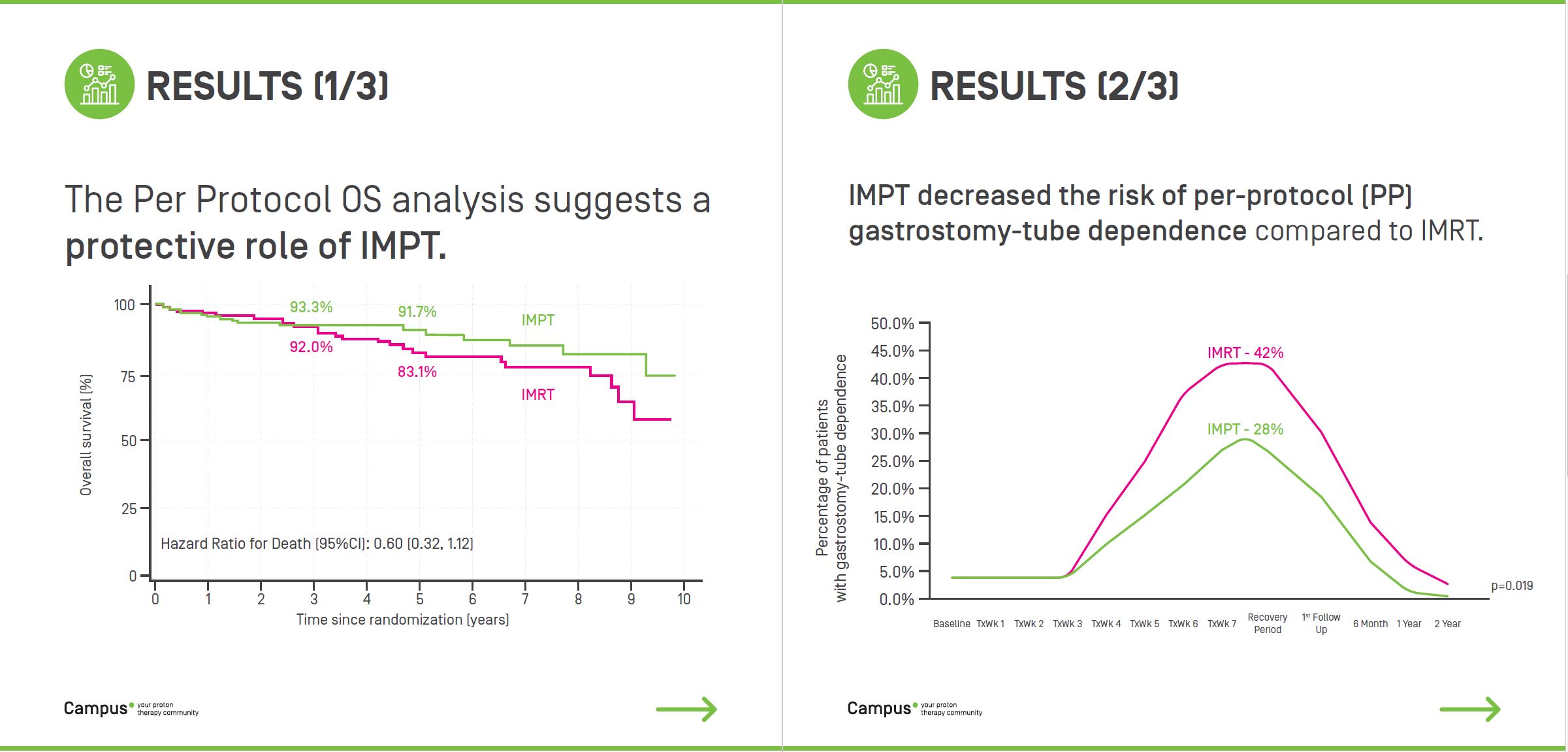
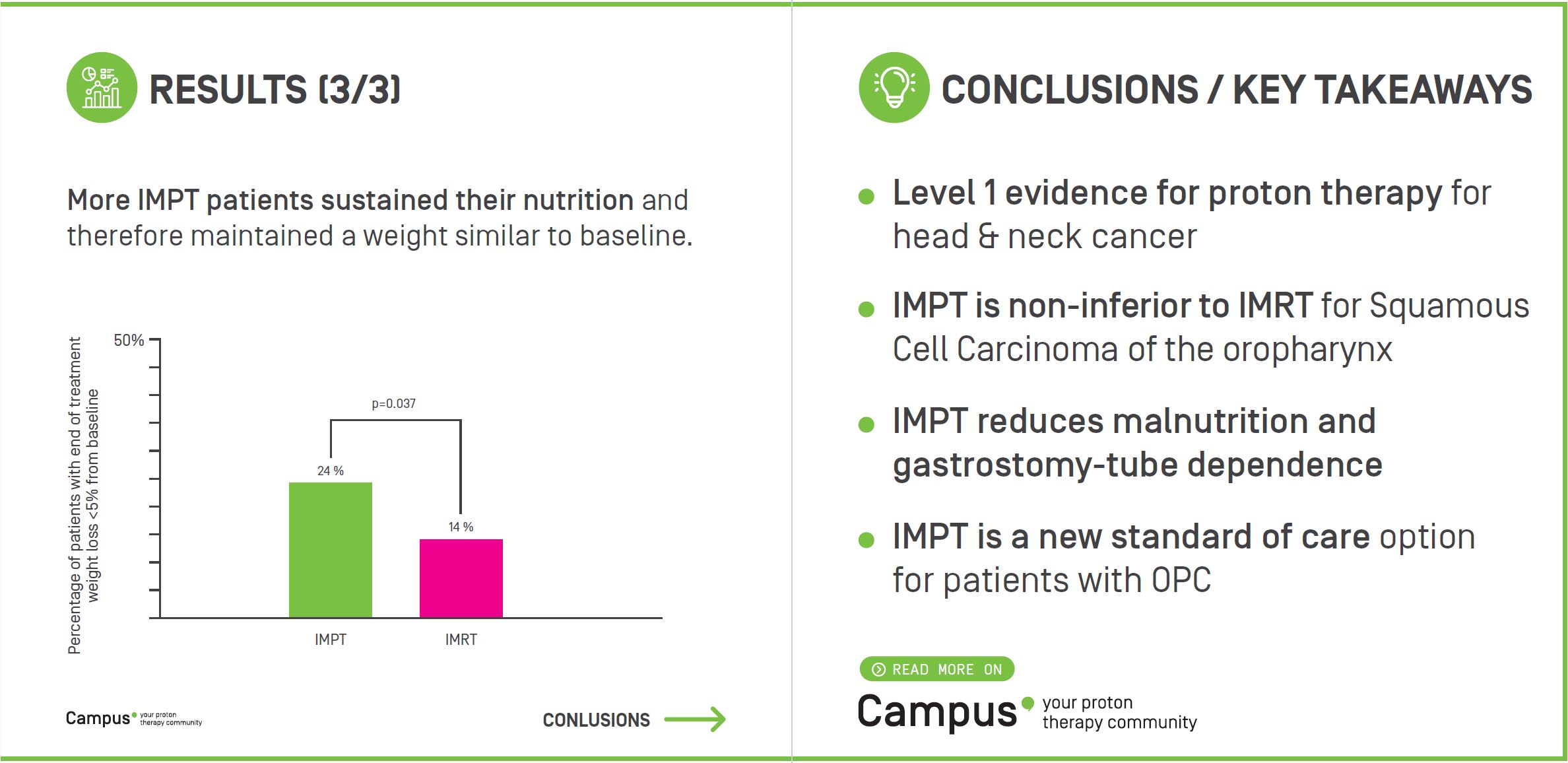
Patients (n=440) were randomized to undergo IMRT(n=219) or IMPT (n=221) at 21 institutions. The median age was 61 years and HPV/p16 was positive in 95%. IC was the initial treatment in 13% of patients. All patients were treated with CRT to 70 Gy in 33 fx with bilateral neck treatment, and post-CRT surgical lymph node dissection occurred in 8%. The median follow-up was 3.14 years. In the ITT analysis, the hazard ratio (HR) for disease progression or death at 3 y was 0.87 (95%CI 0.56,1.35); p=0.006 and the corresponding HR for death (OS) was 0.63 (95%CI 0.36-1.10) suggesting a protective affect with IMPT. In PP analysis, the PFS HR was 0.85 (95%CI 0.52,1.38); p=0.009 and HR for death (OS) was 0.60 (95%CI 0.32-1.12). In the AT analysis, PFS HR was 0.88 (95%CI 0.56,1.37); p=0.007 and the corresponding HR for death (OS) was 0.70 (95%CI 0.40-1.22). For each analysis above, the null hypothesis was rejected and IMPT was non-inferior to IMRT. PP gastrostomy-tube dependence decreased with IMPT vs. IMRT from 42% to 28% (p=0.019), and more IMPT patients sustained their nutrition with end of treatment weight loss < 5% from baseline: 24% vs 14% (p=0.037).
Related contents